Keep taking the tablets, or swap to a low-carb diet.
Praise the Lord and pass the medication!
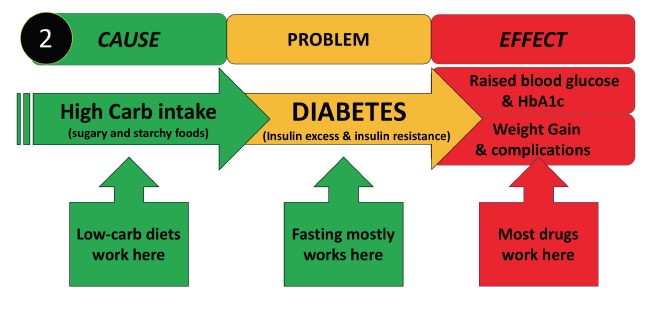
Diets for overweight and diabetes tend to fall into one of two camps: low-cal (energy accountancy) and low-carb (glucose/insulin modulating). Doctors favouring the former are experts in diabetes drug prescribing. Those favouring the latter tend to be experts at de-prescribing.
Just to support that assertion, how about looking at a study that looked at remission rates (how many got better) in people with Type-2 diabetes who were given ‘usual’ management. For ‘usual’ read low-fat, low-cal, plenty of whole-grain foods, regular exercise and of course medicines for their diabetes. The study was conducted in Northern Californian patients of the Keiser Permanente clinics. There were no control subjects for comparison with. They just reported what happened to over 120,000 of their patients. Over the years a few went into remission (got better in other words), but not many did so, and not for long either. This should not be a surprise because the ‘usual’ opinion of doctors treating diabetes is that it is chronic (long-term) and progressive (gets worse as time goes by). Once you got it…. you got it. It isn’t going away
Compare this paper with some data from the Virta Clinic, also in the US. They advocate a low-carb high-health-fat approach and support patients during the programme. Yes, I know. I am comparing apples with pears, or should that be bananas? That cannot be helped as there are basically no long-term randomised trials comparing these approaches. That doesn’t make this exercise invalid. It just ask you to deploy a little common sense.
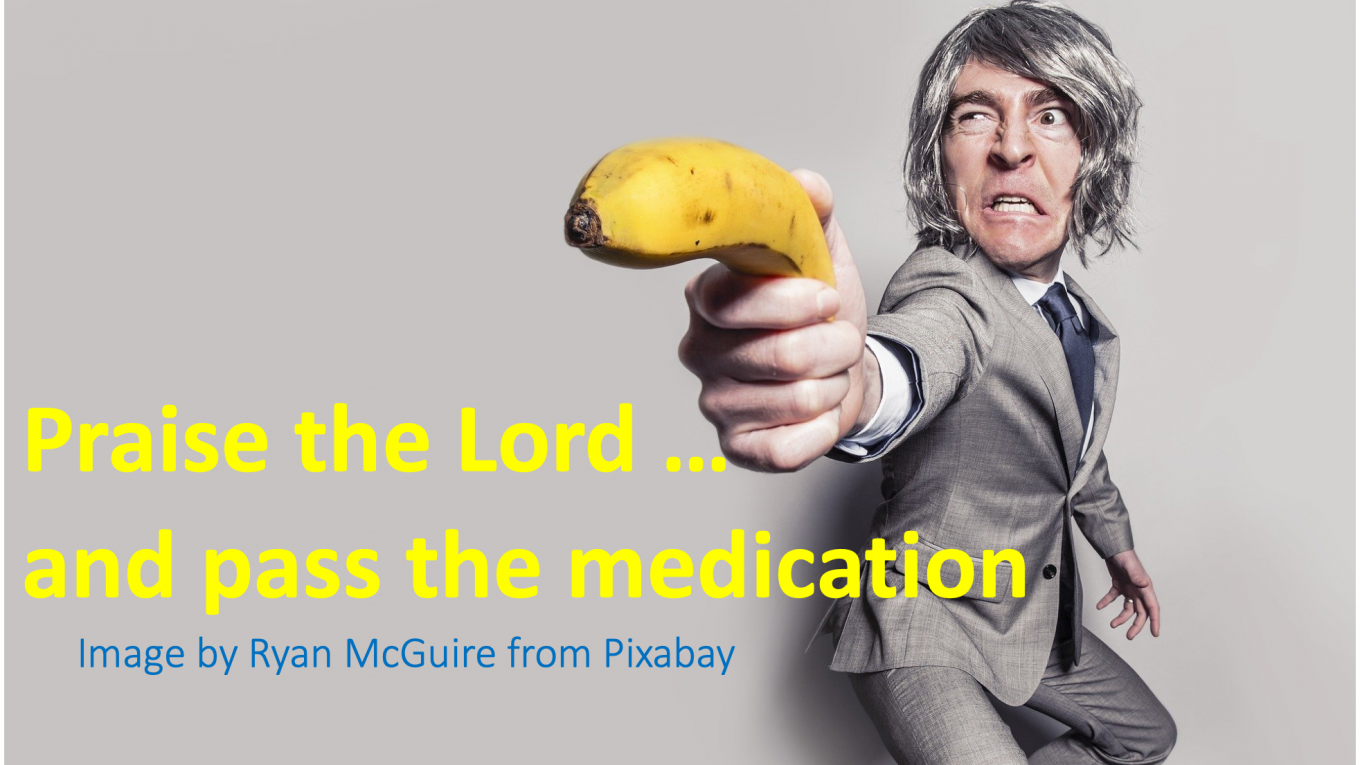
Have a look at this (rather busy) table summarising both publications.
The takeaway headlines are that remission while receiving ‘usual’ management is pretty uncommon. Long-term remission occurred in just one person in ten thousand (0.01%). But now look at the low-carb group. Small numbers but the remission rate is over 50% two years down the line. And, many of those whose diabetes persisted saw an improvement and a reduction in the drugs they were obliged to take. These are dramatic results. So why do we continue with ‘usual’ management? Who benefits from usual management? Not the patient, that’s for sure.